Specialized clinical pathway for rare heart disease proves effective
&width=710&height=710)
Healthy and fit, yet a heart attack…
SCAD is a rare condition that can lead to a heart attack. It occurs about nine times more often in women than in men and usually affects women between 40 and 50 years old who are otherwise healthy. “They are often fit women who have no idea they could have a heart attack,” says interventional cardiologist Ibtihal Al Amri. “It just happens to them, without any clear warning signs beforehand.” Symptoms can start abruptly and may include chest pain or pain between the shoulder blades, shortness of breath, sweating, dizziness, or even fainting.
Different cause, different care
Patients with SCAD are often treated in the same way as those with a typical heart attack, even though the cause is different. A typical heart attack is usually caused by atherosclerosis. Treatment then focuses on opening a blocked artery with a stent and lowering risk factors with medication, such as blood thinners, cholesterol-lowering drugs, and blood pressure medication.
In the case of SCAD, there is no atherosclerosis. Instead, there is a tear or bleeding in the wall of a coronary artery. In many cases, this heals on its own. Procedures or intensive medication can sometimes make things worse or cause side effects, while the underlying problem is not addressed. Unlike a typical heart attack, the risk of SCAD cannot be reduced through lifestyle changes.
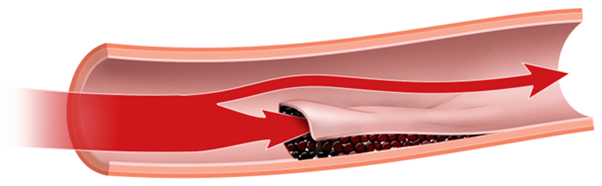 Illustration: Spontaneous coronary artery dissection (source: SCAD Alliance)
Illustration: Spontaneous coronary artery dissection (source: SCAD Alliance)
“With SCAD, leaving it alone is often better than treating it,” says researcher Jin Al-Gully. “Yet for a long time, these patients were treated as if they had a classic heart attack. That did not match what was actually going on. You see that reflected in the medication as well. Patients with SCAD are often prescribed medication for conditions they don’t have, such as high blood pressure or high cholesterol. If you prescribe medication for a problem that isn’t there, you risk side effects and uncertainty. That does not help the patient.”
SCAD clinical pathway
For this reason, the LUMC developed a SCAD clinical pathway based on a conservative and cautious approach. Al Amri explains, “We only place a stent when absolutely necessary and we tailor medication to the individual patient. Aftercare is also an important part of the clinical pathway and focuses on life after the heart attack.”
The SCAD clinical pathway is multidisciplinary. This means that several specialists work together. Besides the cardiologist, this includes a vascular surgeon, a rehabilitation physician, a physical therapist, and a psychologist. “We look beyond the heart,” says Al Amri. “Together, we search for possible underlying causes, such as hormonal changes or abnormalities in the blood vessels. We also take the mental impact seriously.”
This comprehensive approach starts with clear information. Patients learn what SCAD is, what has happened in their bodies, and what they can and cannot expect. Many women feel uncertain after SCAD and find it hard to trust their bodies again. “They are often reluctant to start moving again,” says Al Amri. “We take that fear seriously.” That is why the clinical pathway focuses strongly on personalized support and rehabilitation, in collaboration with Basalt Rehabilitation. Patients are guided to gradually and safely return to their daily activities, with attention to both physical recovery and mental health. “Aftercare is not an ancillary matter in the treatment of SCAD,” Al Amri adds. “It is essential to help people regain confidence in their bodies.”
SCAD clinical pathways is effective
In recent years, the LUMC has conducted research on the SCAD clinical pathway. The results were recently published in the scientific journal Netherlands Heart Journal. They show that this approach effectively meets the needs of SCAD patients.

Patients treated within the SCAD clinical pathway were less likely to receive a stent and were prescribed fewer unnecessary medications. At the same time, outcomes after one year were similar to standard care. There were no extra complications, and the risk of a new SCAD event even seemed lower.
Photo: Ibtihal Al Amri (left) and Jin Al-Gully (right)
The study confirms that a cautious approach, with a strong focus on clear information and aftercare, is safe and better suited to this group of patients. With this publication, the researchers hope other medical centers will adopt the SCAD clinical pathway. This form of care is different but not more complicated,” concludes Al-Gully. “And that makes a real difference for this group of patients.”
What Is Spontaneous Coronary Artery Dissection (SCAD)
In SCAD, a sudden tear or bleed occurs in the wall of a coronary artery. This creates a space between the layers of the vessel wall. As this space fills with blood, it presses on the inside of the artery, making it narrower. As a result, less blood can flow to the heart. This can lead to a heart attack.
You can read more about SCAD and the SCAD care pathway in the Dutch patient brochure.
Want to know more about this research?
Watch this short movie of Jin Al-Gully explaining her research.
Meer weten over dit onderzoek? Bekijk het Engelstalige filmpje waarin Jin Al-Gully meer vertelt over haar onderzoek.

&width=710&height=710)
&width=710&height=710)
&width=710&height=710)
&width=710&height=710)